CFS-FMS and Heart Disease; A few thoughts.
In the articles, "The Heart of the Matter: CFS & Cardiac Issues", it is suggested that CFS may be the result of cardiomyopathy. This latest theory by Dr. Cheney is based on the research study of Dr. Peckerman et al, see "Abnormal Impedance Cardiography Predicts Symptom Severity in Chronic Fatigue Syndrome". There is a lot of good information in the article but I'm not convinced that the theory of heart disease as an originating factor for CFS accurately pertains to the majority of people with CFS-FMS.
In this article I will show that low cardiac output is not necessarily due to cardiomyopathy but that the combined influences of low metabolism, low blood pressure due to low blood volume, and increased resistance to blood flow contribute to low cardiac output. This is not to say that the condition is any less serious, since continued low cardiac output can eventually contribute to the onset of heart disease.
First, what is the normal physiological response to heart disease? In "Human Physiology and Mechanism of Disease" by Guyton we find the following:
Increased Blood volume and Extracelluar Fluid Volume Caused by Heart
Disease:
In congestive heart failure, blood volume may increase 15 to 20 per cent
and extracellular fluid volume sometimes increases by 200 per cent or
more. Initially, heart failure reduces cardiac output and, consequently,
decreases arterial pressure, which causes the kidneys to retain volume
in an attempt to return the arterial pressure and cardiac output toward
normal. In myocardial failure, heart valvular disease, and congenital
abnormalities of the heart, an important circulatory compensation is an
increase in blood volume, which helps to return cardiac output and blood
pressure to normal. [2:pg.247]
If people with CFS-FMS were having heart failure it is logical to
expect that there would be an increase in blood volume, the normal
physiological response to heart disease. However, the research of
Dr. Streeten and Dr. Bell found just the opposite; People with CFS
tend to have decreased blood volume.
( see
Evaluating
Blood Volume Studies - Some Thoughts
and
Circulating Blood Volume )
What is "Q"?
In the "Heart of the Matter" article, there is much talk of "Q", but it is
not clearly explained what "Q" is, other than that it is a measure of the
rate of blood flow. In this case cardiac output.
It may help to gain a better understanding of "Q" and the factors that
influence the value for "Q".
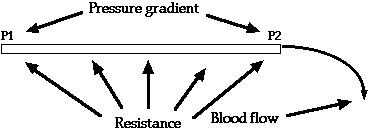
In the equation for Ohm's Law, "Q" is the variable commonly used to represent the rate of blood flow.
delta(Pressure) (P1 - P2)
Q = ________________ = _________
Resistance R
|
Where Q is blood flow, (P1 - P2) is pressure difference (for example, if you wanted to calculate blood flow between the arteries and veins, P1 would represent mean arterial pressure and P2 would represent venous pressure), R is the resistance to flow.
Many people likely think that it is the pumping action of the heart that causes blood to flow. Actually it is the pressure gradient that causes blood to flow. The heart performs the essential function of pumping blood from the veins back into the arteries to maintain arterial blood pressure, without which blood would cease to flow (assuming that arterial pressure is greater than venous pressure).
The flow of blood in the circulatory system could be likened to rain waters and waters trickling down from mountains, flowing into streams, flowing to rivers, flowing to the sea. In the case of waters on earth, it is the force of gravity that causes the waters to move to the sea. In the circulatory system it is the pressure gradient that causes blood to flow to the veins and back to the heart.
A normal mean arterial pressure is about 100 mmHg. and venous pressure
is about 0 mmHg. Substituting these values for P1 and P2 in Ohm's Law
we would get:
( Note: The mean, or average, arterial pressure is calculated by adding
systolic blood pressure and diastolic blood pressure and dividing the sum by 2. According to information on
[another website],
the average blood pressure for young people is 120/80 mmHg and the
average blood pressure for old people is 140/90 mmHg. So, the mean
arterial pressure for a young person is (120 + 80) / 2, or 100 mmHg.
(P1 - P2) (100 - 0) 100 60 sec
Q = ________ = _________ = ___ = 100 ml/sec * ______ = 6 liters/min
R 1 1 1 min
|
( Note: The values used in these examples are approximations. They are used for demonstration purposes to show how changes in the different variable values affect the value for blood flow, "Q", and subsequently cardiac output. It is not intended to imply that these values are common in people with CFS-FMS. )
Normal blood flow in the body at rest is about 5 liters/min, so the value of "R" for the body in this case may be calculated as being closer to 1.2. The value of "R" will be explained in more detail later.
(P1 - P2) (100 - 0) 100
Q = ________ = _________ = ___ = 83.3 ml/sec = 5 liters/min
R 1.2 1.2
|
If pressure in the veins (P2 in our example) were to rise to 100 mmHg. the pressure difference would be zero, 100 - 100 = 0. There would be no blood flow. This may give a better appreciation for the importance of blood pressure and the many mechanisms in the body designed to maintain and protect blood pressure.
The "Distribution of Pressures and Volumes" graph at another website, shows the differences in blood pressure and blood volume at different locations in the circulatory system.
The heart normally plays a permissive role in cardiac output regulation. That is, it is capable of pumping a certain amount of blood each minute and therefore will permit the cardiac output to be regulated at any value below this given permitted level. The normal human heart that is not stimulated by the autonomic nervous system permits a maximum heart pumping of about 13 - 15 liters per minute, but the actual cardiac output under resting conditions is only approximately 5 liters per minute because this is the normal level of venous return. Therefore, it is the peripheral circulatory system, not the heart, that sets this level of 5 liters per minute. [2:pg.188]
The whole theory of normal cardiac output regulation is that the tissues control the output in accordance with their needs... It is not the heart that controls the cardiac output under normal conditions; instead, the heart plays a permissive role that allows the tissues to do the controlling. [2:pg.189]
The most important factor that controls the local blood flows in the individual tissues is the metabolic rates of the respective tissue. Therefore, venous return and cardiac output are normally controlled in relation to the level of metabolism of the body. However, it is essential that arterial pressure be maintained at a normal level if changes in metabolism are to regulate cardiac output. [2:pg.189]
Units of Resistance. Resistance is the impediment to blood flow in a vessel, but it cannot be measured by any direct means. Instead, resistance must be calculated from measurements of blood flow and pressure difference in the vessel. The rate of blood flow through the circulatory system when a person is at rest is close to 100 ml./sec., and the pressure difference from the systemic arteries to the systemic veins is about 100 mmHg. Therefore, in round figures the resistance of the entire systemic circulation, called the total peripheral resistance, is appoximately 100/100 or 1 PRU (Peripheral Resistance Unit). In some conditions in which the blood vessels throughout the body become strongly constricted, the total peripheral resistance rises to as high as 4 PRU, and when the vessels become greatly dilated it can fall to as little as 0.2 PRU. [2:pg.144]
Now that we have a little better understanding of pressure and resistance, lets plug a few values into the variables in the equation for Ohm's Law to see how it affects cardiac output, "Q".
Many people with CFS-FMS tend to have lower blood pressure. For this example let's use the blood pressure of 110/60 which is reported by one person w/CFS-FMS here. Calculating the mean arterial pressure, (110 + 60)/2 = 85 mmHg. plugging this value into the formula we get
(P1 - P2) (85 - 0) 85
Q = ________ = _________ = ___ = 70.8 ml/sec = 4.25 liters/min
R 1.2 1.2
|
There is a direct relationship to arterial blood pressure and "Q". As arterial blood pressure ("P1") lowers, the value for "Q", blood flow, also lowers. Likewise, if mean arterial pressure, "P1", rises there would be a corresponding rise in cardiac output, "Q" (assuming that the values for "P2" and "R" remain the same).
"Work looking at vascular perturbations in CFS in adolescents in relation
to chronic orthostatic intolerance was presented by J Stewart (NY). He
found that leg circumference tends to be larger in CFS patients on
standing, and resting venous pressure was higher in CFS than controls."
(see Reports On AACFS Conference In Seattle, January 2001)
I have not found any specific values to use for illustration so for our example let's make one up; Let's say that venous pressure is risen from 0 mmHg. to 5 mmHg. Now let's factor that into the equation for Ohm's Law and see how it affects "Q".
(P1 - P2) (85 - 5) 80
Q = ________ = _________ = ___ = 66.7 ml/sec = 4.0 liters/min
R 1.2 1.2
|
There is an inverse relationship to venous blood pressure and "Q", as venous blood pressure (P2) rises, the value for "Q" lowers.
Now lets see how a change in resistance can affect "Q". The text [2] indicates that in strongly constricted states the value of "R" could be as high as 4. I suspect that resistance this high is for localized tissue blood flow. If systemic resistance were ever this high its affect would reduce blood flow so much that the body could not survive. In our example so far we have been using a value of "R"=1.2, what is the affect on "Q" if "R" increases to 1.3 ?
(P1 - P2) (85 - 5) 80
Q = ________ = _________ = ___ = 61.5 ml/sec = 3.7 liters/min
R 1.3 1.3
|
We find an inverse relationship to resistance and "Q"; As resistance ("R") increases, "Q" decreases. Conversely, a decrease in systemic resistance will cause an increase in "Q".
Low Blood Volume:
Factors that decrease the venous return. The most common cause of
decreased venous return is (a) diminished blood volume, but venous
return also can be reduced as a result of (b) decreased vasomotor tone
or (c) obstruction to blood flow at some point in the circulation,
especially in the venous return pathway to the heart. [2:pg.174]
Since cardiac output is largely determined by the amount of blood returning to the heart we see that low blood volume has a great affect on reducing cardiac output.
As blood volume decreases, blood pressure will drop as a result. The vascular system can compensate for this drop in blood pressure by increasing vasoconstriction. But over time, as the adrenals become exhausted, I suspect that the means by which vasoconstriction can maintain blood pressure may diminish.
Whenever blood flow to the kidneys diminishes, renin is secreted and
angiotensin is formed. The angiotensin in turn causes widespread
vasoconstriction throughout the body with consequent greatly increasing
total peripheral resistance. [1:pg.180]
(remember, in Ohm's law, as "R" increases, "Q" decreases.)
The findings of research on microcirculation in fibromyalgia is interesting. (see "Microcirculation abnormalities in patients with fibromyalgia") The person with FMS, as compared to healthy control subjects, has fewer capillaries and significantly more capillary dilatations. A decrease in the number of capillaries would cause an increase in "R". (an increase in "R" causes a decrease in "Q")
The following was written specifically about the heart muscle but I
think that it applies to other muscle tissue as well.
The substance with the greatest vasodilator propensity is adenosine. In the presence of very low concentrations of oxygen in the muscle cells, a large proportion of the cell's adenosine triphosphate (ATP) degrades to adenosine monophosphate; then small portions of this are further degraded to release adenosine into the tissue of the heart muscle. After the adenosine causes vasodilation, much of it is reabsorbed back into the cardiac cells to be reused. [2:pg.183]
This would explain the capillary dilatations found in the microcirculation of people with FMS reported above.
It appears that the cellular substances that signal a need for more oxygen and nutrients cause capillary dilatation which better assures that blood flow to the area will increase, providing the needed nutrients to the tissue. However, the dialatation is countered by the body's attempt to maintain blood pressure by reducing the number of capillaries. One affect that reducing the number of capillaries will have is that it will increase resistance. (An increase in "R" causes "Q" to decrease.)
Orthostatic Intolerance:
Though not directly related to cardiac output, since we've touched
upon low blood volume, I'd like to diverge for a moment to speculate on
the common problem of orthostatic intolerance in people with CFS-FMS.
"Role of the Volume Receptors in Blood Volume Control. "Volume receptor"
reflexes help to control blood volume. The volume receptors are stretch
receptors located in the walls of the right and left atria. When the
blood volume becomes excessive, a large share of this volume accumulates
in the central veins of the thorax and causes increased pressure in the
two atria. The resultant stretch of the atrial walls transmits nerve
signals into the brain, and these in turn elicit responses that accelerate
the return of blood volume to normal. The various reponses that occur
include the following:
- The sympathetic nervous signals to the kidneys are inhibited, thus
slightly to moderately increasing the rate of urinary output.
- The secretion of antidiuretic hormone by the supraopticohypohyseal
system is reduced, allowing increased water excretion by the kidneys.
- The peripheral arteriols throughout the body are dilated because of reflex reduction of sympathetic stimulation, thus increasing capillary pressure and allowing much of the excess blood volume to filter temporarily into the tissue spaces for a few hours until the excess fluid can be excreted through the kidneys.
In most instances, these volume receptor reflex effects can cause the blood volume to return almost all the way to normal within an hour or so, but the final determination of the precise level to which the blood volume will be adjusted is still a funtion of the basic volume control mechanism discussed above. The reason is that over a period of one to three days the volume receptors adapt so completly that they no longer transmit any corrective signals. Therefore, they are of value only to help readjust the volume during the first few hours or days after an abnormality occurs but not for long-term monitoring of volume or for precise adjustments of the long-term level of blood volume." [2:pg.271]
The Low Blood Pressure Abstracts (on another website) describe the results of tilt table tests with people with CFS-FMS. Basically, when the person w/CFS-FMS is put on a tilt table and laying in the prone position, all is okay but when the person is then tilted upright they tend to get light headed and faint due to lack of blood flow to the brain. All the subjects in the studies also experienced a worsening of widespread fibromyalgia pain. The person did not undergo any strenuous exercise but is experiencing an increase in pain as a result of laying flat and being tilted upright. What's up with this?
Let's speculate what may be happening in the tilt table test. Laying flat on the back, the heart is gettting plenty of blood delivered to it. Maybe, if the volume receptors have adapted to a lower blood volume and due to an increase in venous pressure (found in people with CFS-FMS) the volume receptors now sense that there is more blood being delivered to the heart. This could cause the volume receptor reflex to signal an increase in blood volume. What is a normal physiological response to this? As shown in no. 3 above, one response is to dialate the peripheral arterials.
The person is then tilted back to an upright position. With the arterials now dialated, the person has lost blood pressure. The researchers found an average drop in systolic blood pressure of at least 25 mmHg and no associated increase in heart rate (abstract II). Add to this the affect that gravity has of pooling blood to the lower extremities and the result is reduced blood flow to the brain. The body naturally responds by fainting. This physiologic response gets the head lower so that blood flow can return to the brain. The body then attempts to restore systemic blood pressure through vasoconstriction. There is likely a great release of norepinephrin into the blood to increase vasoconstriction.
Norepinephrine and Epinephrine. Norepinephrine is an especially powerful vasoconstrictor hormone; epinephrine is less so and in some instances even causes mild vasodilation. When the sympathetic nervous system is stimulated during stress or exercise, the sympathetic nerve endings release norepinephrine, which excites the heart, the veins, and the arterioles. The nerves also cause the adrenal medullae to secrete both norepinephrine and epinephrine into the blood. These hormones then circulate in the blood and cause almost the same excitatory effects on the circulation as direct sympathetic stimulation, thus providing a dual system of control. [2:pg.146]
A person w/FMS on [another website] observed that when experiencing a fibromyalgia flare, blood pressure goes up. By fibro flare, I'm assuming an increase in wide-spread body pain. It may be that a release of norepinephrine is triggering vasoconstriction which accounts for the increase in blood pressure and which may be responsible for the subsequent pain.
This reasoning is supported by the conclusion of the study outlined in the article "Norepinephrine-Evoked Pain in Fibromyalgia?".
I suspect that it is the effects of norepinephrine and not the substance itself that causes the pain. That is, oxygen deprivation as a result of too much vasoconstriction restricting blood flow is causing the pain, rather than the norepinephrine itself.
An increase in arterial blood pressure, according to Ohm's Law, would normally result in an increase in blood flow, or cardiac output. However, in this case, since the blood pressure is being increased by an increase in vasoconstriction, vasoconstriction will cause an increase in resistance ("R"), the increase in "R" could negatively counter any increase in "Q" that would normally result from an increase in arterial blood pressure.
Use It or Lose It:
While cardiomyapathy may not be the cause of the low cardiac output the
condition of low blood volume is still serious. As low metabolism
contributes to low cardiac output, the low blood flow then causes a
further drop in metabolism. The additional decline in metabolism then
contributes to a further lowering of cardiac output. This causes a further
decrease in blood volume, and so on, and so on ... It is a slow downward
spiral.
If you look at the data presented in Dr. Peckerman's research you will see that the stroke volume (fig.1) and cardiac output, "Q" (fig.2) in the "less-severe" CFS subjects is very similar to the stroke volume and cardiac output of the normal, healthy, control subjects.
The research of Dr. Streeten and Dr. Bell did not show that low blood volume was a problem in all their patients with CFS. The symptom of low blood volume was applicable to about eighty percent of their patients.
What is likely happening is that in the early stages of CFS-FMS there is no problem with blood volume but only with blocks to metabolism. Due to impaired (low) metabolism in the tissue the body does not sense a need to deliver as much blood to the tissue. Over time blood volume is decreased; The reduction in demand for blood slowly creates a condition in which blood volume further decreases. This Contributes to a slow decline of the condition. Notice in fig.1 that the subjects in Dr. Peckerman's study catagorized as having "severe" CFS symptoms have a much lower stroke volume and lower cardiac output, "Q".
Something else to consider:
You've just read that low metabolism can lead to low blood volume; Here
is something else to think about. When there is reduced blood flow to the
kidneys, the kidneys detect the lower blood volume and are supposed to make
adjustments to restore blood volume back to normal.
Current treatment options for pain associated with fibromyalgia include physical therapy, nonsteroidal anti-inflammatory drugs and muscle relaxants that may provide temporary relief.[ ref.]
Afferent arteriolar vasodilation in the glomerulus is mediated by prostaglandins. A loss of glomerular capillary pressure is possible when nonsteroidal anti-inflammatory drugs (NSAIDs) are consumed since they function by inhibiting prostaglandin synthesis. This drug-induced renal insult is compounded in patients with comorbidities that decrease renal perfusion or lead to hypovolemia.[ ref.]
Long-term use of large amounts of NSAIDs can cause stomach ulcers or kidney damage.[ ref.]
NSAIDs affect renal physiology by inhibiting cyclo- oxygenase and the synthesis of vasodilatory prostaglandins resulting in acute intrarenal hemodynamic changes that can cause reversible deterioration in the renal function of susceptible individuals. Thus, in individuals with decreased renal blood flow, impaired renal function, or hypovolemia, the use of NSAIDs can produce an increase in serum creatinine concentrations and a decrease in creatinine clearance that may progress to acute renal failure, but which is reversible by stopping the drug.[ ref.]
non-steroidal anti-inflammatory drugs are potentially dangerous in situations with even moderate volume depletion.[ ref.]
In Dr. Peckerman's study, the people with "less severe" CFS had blood flow similar to that of the healthy control subjects. Assuming that the "severe" CFS subjects have had the condition for much longer they may have been prescribed NSAIDs, which over time could have contributed to some kidney damage. I wonder what part, if any, the taking of these medications may have played in the reduction of blood volume in the people with "severe" CFS symptoms. It is the job of the kidneys to help maintain blood volume levels. It's something to think about.
If you do suspect low blood volume, and are taking NSAIDs, you may want to discuss the possible risks with your doctor. The good news, according to the above information, is that any damage that may have been done by NSAIDs appears to be reversible.
Metabolism
The cardiac output usually remains almost proportional to the overall
metabolism of the body. That is, the greater the degree of activity of
the muscles and other organs, the greater also will be the cardiac
output. [2:pg.187]
For each degree rise in temperature above 98.6 F. the basal rate is increased about 7 percent. For example, with a body temperature of 103.6 F., which is 5 degrees above normal, the basal metabolism will increase 35 per cent. Malnutrition will lower the basal metabolism, depending upon the degree of malnutrition. [3:pg.197]
The above information is corroborated with the following:
Body Temperature/Health. For every increase of 0.5C in internal
temperature of the body, the BMR increases by about 7 percent. The
chemical reactions in the body actually occur more quickly at higher
temperatures. So a patient with a fever of 42C (about 4C above normal)
would have an increase of about 50 percent in BMR.
(see "Basal Metabolic Rate Determines How Many
Calories Burned")
Temperature also has a significant effect on blood viscosity. As temperature decreases, viscosity increases. Viscosity increases approximate 2% for each degree C. decrease in temperature. (see "Cardiovascular Physiology Concepts")
Increased blood viscosity causes increased resistance. As has been shown in the above examples using Ohm's Law, an increase in resistance causes decreased blood flow, "Q", which equates to decreased cardiac output.
A Few Logical Conclusions:
Most people with CFS-FMS have a body temperature about a degree Farenheit
or more below the generally accepted normal temperature of 98.6 F. Via
extrapolation we can approximate that a person with a temperature of 97.6 F. has
a decrease in metabolism of about 7 per cent. As we have learned, there is
a correlation between metabolism and cardiac output; As metabolism
decreases so too does cardiac output. Over time, a lowered
metabolism contributes to a lowering of blood volume, and lowered blood
volume contributes to further lowering of metabolism.
Endotoxin. Endotoxin is a toxin released from the bodies of dead gram-negative bacteria in the intestines. Diminished blood flow to the intestines causes enhanced formation and absorption of this toxic substance. [2:pg.176] (a little off the topic but I thought it interesting.)
With low blood volume there appears to be a delicate balance in distribution of blood flow; A balance between things that cause vasodialation and things that cause vasoconstriction. Anything that upsets this balance can produce compensating reactions which may appear to be negative reaction.
For example, the tilt table test. The subject with CFS-FMS has low blood volume which is balanced with the just the right amount of vasoconstriction to maintain blood pressure, the person is tilted to a horizontal position, the body detects an increase in blood volume and responds accordingly; Sympathetic vasoconstriction controls are lessened and arterials dialate. Then when the person is put upright again, vasoconstriction cannot respond quickly enough. The person gets faint from lack of blood flow to the brain. The compensating release of norepinephrine then causes pain in the body.
This is a chicken and egg conundrum, In some people it may be that low blood flow due to heart damage has resulted in CFS symptoms. I believe that for the majority of people with CFS-FMS, it is impaired metabolism that is responsible for low blood flow, resulting in low cardiac output and eventually low blood volume. As is pointed out several times in this article, it is metabolism that largely influences cardiac output.
Increased Blood Volume Caused by Increased Capacity of the
Circulation
Any condition that increases vascular capacity will also cause the blood
volume to increase to fill this extra capacity. An increase in vascular
capacity initially reduces mean circulatory filling pressure, which
leads to decreased cardiac output and decreased arterial pressure.
[2:pg.247]
If cardiac output is determined by metabolism, it is logical to think that increasing metabolism would help to increase cardiac output. One way to help increase metabolism is to raise the body's temperature. The FIR sauna is beneficial in raising the body temperature.
An affordable means to accomplish this is to use two free standing far infrared heaters in the bathroom. As is described in the article " The Bathroom for FIR Sauna".
Part of the Remedy:
Regular use of FIR sauna is helpful in raising the body temperature which helps to increase metabolism, increase circulation, and lower blood viscosity, all of which help to increase cardiac output. Over time, the kidneys should adjust to the need for more blood to meet the demands for the increase in metabolism and slowly restore blood volume.
I took my blood pressure reading the other day at one of those free BP stations in a local supermarket. My blood pressure was 121/79. My heart rate was 64 BPM. I may be aging on the outside, but my blood pressure still appears to be like that of a young person. I've been using FIR sauna about 1X/week for the last 6 years. I would guess that I'm in better health than many people half my age. Unfortunately, this speaks more for the large number of young people that are in poor health. In the long run, the monetary investments that I've made in health aids over the years have paid for themselves many times over. (Note: the point that I am trying to make here is that if there are long term adverse affects that may come from FIR sauna use, I've not found them yet. My body, like everyone elses, will eventually fail and return to dust. Hopefully I will not have any more need for it then.)
There are some precautions to take using the FIR sauna, especially if the body may be in a dehydrated state (hypovolemic) or depleted of some minerals, but if you start out slow and do not push it and take necessary precautions, which I can tell you about from the experience of those that have encountered problems and shared their observations, regular use of FIR sauna to increase metabolism is, in my opinion, part of the answer to reversing symptoms of CFS-FMS. It is not the whole answer but it is a key part of the program.
If you would like to learn more, the information on the website at http://www.xmission.com/~total/temple/index.html may be of interest. Also, you are invited to join us on the yahoogroup CFS-FMS_FIRST-Aid where you can learn from the first hand experiences of those following the program.
If you have any questions please feel free to ask. Post them in the yahoogroup or send me an email. I hope that the information in this article has been of some help in your better understanding of "Q".
All the best,
Jim
email: clements@xmission.com
1. "Human Physiology and Mechanisms of Disease" Arthur C. Guyton, M.D., third edition, 1982.
2. "Human Physiology and Mechanisms of Disease" Arthur C. Guyton, M.D., sixth edition, 1982.
3. "Principles of Nutrition", E.Wilson, K.Fisher, and M.Fuqua, second edition, 1966.